Executive summary
A rare Bundibugyo Ebola outbreak in eastern Democratic Republic of the Congo (DRC) has escalated rapidly. The World Health Organization has declared the situation a Public Health Emergency of International Concern. As of the latest official updates, 695 confirmed cases and 138 deaths span the DRC and neighbouring Uganda. This crisis matters to business leaders because it threatens regional stability, supply chains, humanitarian security, and the investment climate. Moreover, the outbreak exposes critical gaps in medical countermeasures, surveillance and cross-border response. This analysis explains the public-health facts succinctly. It then reads the economic, geopolitical and strategic implications for Nordic and global decision-makers. Finally, it proposes actionable priorities and medium-term scenarios.
Epidemic snapshot and immediate trajectory
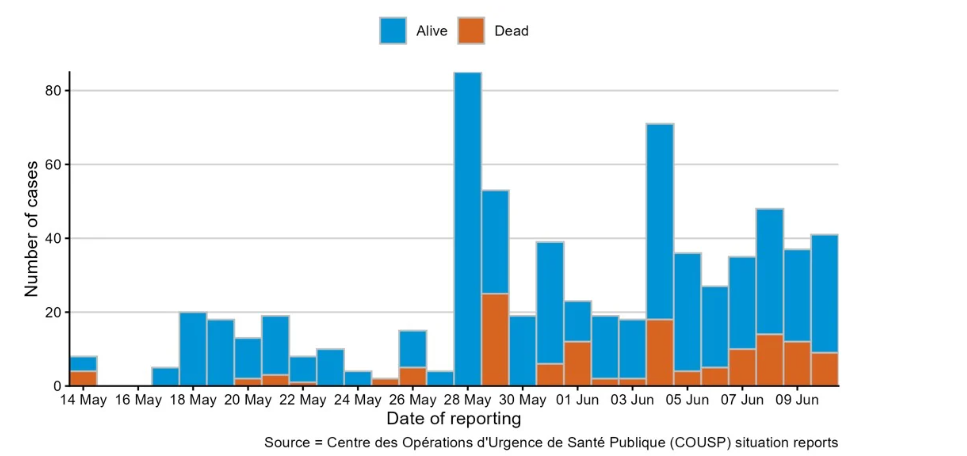
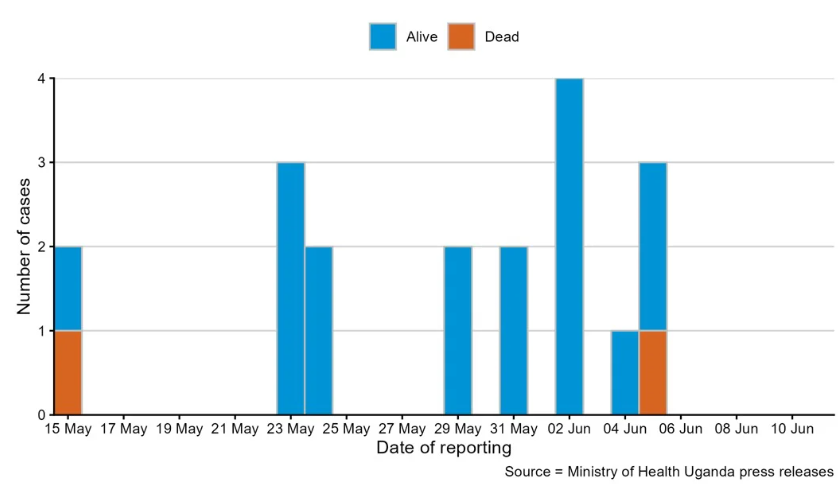
According to aggregated WHO reporting, the outbreak shows accelerating indicators. Total confirmed cases number 695 across both countries. Confirmed deaths total 138. The DRC records 676 cases and 136 deaths. Uganda has reported 19 cases and two deaths. Recent increases partly reflect a large backlog of laboratory samples cleared by expanded testing. Consequently, short-term case counts surged. Importantly, Ituri Province remains the dominant hotspot, accounting for roughly 93–94% of infections. Transmission corridors now reach across more than 1,000 kilometres, from Aru in northern Ituri down through North and South Kivu provinces. Cross-border cases have been documented in Uganda. An evacuated United States national required isolated treatment in Germany. In short, containment remains fragile.
Why this outbreak is unusually difficult
Three features make this Bundibugyo outbreak uniquely hard to contain. First, there are no licensed vaccines or targeted therapeutics for the Bundibugyo strain. Therefore, clinicians must rely on supportive care alone. Second, social and security conditions complicate response operations. Conflict, artisanal-mining mobility and crowded internally displaced person camps impede safe contact tracing. Third, community resistance and distrust have at times led to violent pushback. For example, residents in some localities attacked treatment sites and removed deceased relatives for traditional burials. Together, these factors widen transmission windows and constrain timely isolation.
Clinical profile and public-health consequences
Bundibugyo virus disease presents as an acute viral haemorrhagic fever. Clinically, it often begins with non-specific influenza-like symptoms. It then progresses to severe gastrointestinal loss, dehydration, and in later phases, a characteristic maculopapular rash. Historically, Bundibugyo’s case fatality rate sits lower than Ebola Zaire. For this outbreak, the DRC CFR is currently estimated at about 20.1%. However, health agencies caution that under-ascertainment and unregistered historical deaths likely underestimate true mortality. Importantly, patients become infectious only after symptom onset, which offers an operational window for targeted surveillance and isolation.
Economic exposure: mining, trade and regional commerce
The eastern DRC is economically strategic. It underpins extraction of cobalt, copper and other minerals central to global energy transition supply chains. Consequently, the outbreak threatens operations in several ways. First, workforce absenteeism and travel restrictions can depress production. Second, security-related shutdowns and community unrest can interrupt logistics and port throughput. Third, investor risk premia may rise for assets with on-the-ground exposure. For Nordic investors and industrial buyers, this means reassessing counterparty resilience and supply‑chain diversification. Further, national travel advisories and corporate duty-of-care obligations will affect business continuity planning.
Humanitarian and social stability risks
This outbreak compounds pre-existing humanitarian stress. Regions affected already host large internally displaced populations. Therefore, health, food and shelter deficits risk intensifying. Moreover, the convergence of infectious disease, insecurity and poverty heightens the danger of protracted instability. For policymakers, the take-away is clear. Short-term containment must integrate humanitarian access, community engagement and security assurances. Otherwise, health interventions will be repeatedly undermined.
Gaps in countermeasures and innovation opportunities
Clinically relevant approved vaccines and monoclonal antibodies target Ebola Zaire strains, not Bundibugyo. As a result, treatment remains supportive. This gap creates a dual policy and market signal. From a policy angle, international donors and regulators should prioritise strain‑agnostic therapeutic research and accelerated trials. From an industry angle, the crisis opens opportunities for diagnostics, rapid-test developers and next‑generation antivirals. Nordic life-science firms and medtech startups could contribute scalable innovations. However, investors must balance commercial opportunity with ethical considerations and regulatory complexity.
Regional geopolitics and donor dynamics
International response efforts are already mobilising. The Africa Centres for Disease Control and Prevention and the WHO have outlined continental support frameworks. External actors, including the US CDC, have issued travel advisories for affected provinces. Donors will likely face pressure to scale funding and personnel quickly. Geopolitically, the outbreak could sharpen competition among external partners for influence through humanitarian assistance. For Nordic governments, this suggests a strategic opportunity to align aid with regional stability goals. In practice, targeted support for diagnostics, community engagement and logistics may offer outsized returns in both humanitarian and geopolitical terms.
Business implications and recommended actions
For executives and investors with exposure to the region, immediate and pragmatic steps are essential. First, conduct rapid operational risk assessments focused on personnel, logistics and contractual continuity. Second, diversify supply chains for critical minerals and components. Third, enhance employee health protocols and evacuation plans with clear thresholds. Fourth, engage with insurers to clarify coverage for epidemic-related disruption. Fifth, for asset owners, strengthen security protocols in coordination with humanitarian actors. Finally, consider supporting local public-health capacity as part of corporate social responsibility and stability strategy.
Longer-term trends and scenarios
Looking beyond the immediate crisis, expect three durable trends. First, donors and markets will push for broader-spectrum pan-filovirus countermeasures. Second, private sector investment in outbreak surveillance and digital contact tracing will grow. Third, companies with resilient, diversified African strategies will outperform peers when instability recurs. Conversely, firms that maintain concentrated exposure to fragile corridors will face sustained risk-premia. In economic terms, commodity buyers should prepare for episodic regional disruptions rather than one-off events.
Why now: the confluence of risk factors
This outbreak demands attention because it converges public-health risk with key economic nodes. It occurs during a period of heightened commodity demand and constrained supply. Moreover, the absence of specific countermeasures amplifies uncertainty. Therefore, action now can materially reduce both humanitarian harm and financial exposure.
Conclusion: strategic perspective for decision-makers
The Bundibugyo outbreak in eastern DRC is a serious and rapidly evolving crisis. It combines epidemiological complexity with economic and geopolitical consequences. For Nordic and international stakeholders, the policy imperative is twofold. First, support immediate containment through funding, logistics and community engagement. Second, accelerate investments in medical countermeasures, diagnostics and resilient supply‑chain design. Doing so will protect both lives and long-term commercial interests.
Editorial Outlook
Future follow-up coverage should examine how corporate supply chains adapt to recurrent health-security shocks in central Africa. Specifically, we propose an investigative piece on mining-sector resilience, insurance market responses, and innovation paths for pan-filovirus countermeasures. The follow-up should include interviews with Nordic corporate leaders, biotech investors, and regional public-health officials.
Reader engagement
Nordic Business Journal welcomes dialogue with executives, investors, policymakers, and entrepreneurs on this topic. Please contact our editorial team for briefings, partnerships, and insights tailored to your sector. We also invite readers to share operational case studies and risk-management practices for publication.
References
– World Health Organization, Disease Outbreak News: Bundibugyo virus disease — Democratic Republic of the Congo and Uganda. (Latest aggregated reporting).
– Africa Centres for Disease Control and Prevention, Continental Response Framework announcement, 2026.
– US Centers for Disease Control and Prevention, Travel Advisory: Ituri, North Kivu and South Kivu provinces, 2026.
– Peer-reviewed literature on Bundibugyo virus clinical characteristics and historical case fatality ranges (selected reviews and field reports).
– Sector briefings on DRC mining corridors and supply-chain exposure (industry analyses and trade data summaries).
Note: Numerical figures and operational details reflect the most recent aggregated public health updates at time of publication. Readers should consult official WHO and national health ministry channels for real-time guidance.